Targeted cancer therapies for every patient who could benefit.
Variant classification for patient stratification, label expansion, and resistance anticipation.
Today, most targeted cancer trials enrol only patients carrying clear loss-of-function variants — a fraction of the population that could respond to treatment. Patients with Variants of Uncertain Significance are excluded, and even well-established pathogenic variants are stratified more coarsely than the underlying biology demands. We use geneSlice™ to classify gene variants at scale, so drug developers can stratify patients more accurately, expand trial eligibility, and anticipate resistance — across any cancer indication.
Clinical uncertainty for the majority of variants.
For clinically actionable cancer genes, clearly pathogenic variants represent only a fraction of patients with variants in the target. The remainder — splice-site variants, late-gene frameshifts, and the large class of missense VUS — sit in clinical uncertainty. Their functional impact is uncharacterised. They are excluded from trials and lose a treatment opportunity that variant-level data could unlock.
Three angles on variant data
Variant classification for trial recruitment & stratification
Functional databases of variant-level drug sensitivity across your target gene. Trial recruitment can extend beyond clear loss-of-function (LOF) variants to include functionally validated VUS; stratification can match variant biology to drug response. This is the core Oncology service.
Synthetic lethal target validation & per-variant studies
For target discovery work and per-variant arrayed studies — including full cell viability curves and dose-response — see Custom Services.
Resistance anticipation
For residue-level resistance mapping of a specific compound, see Compound–Target Assay.
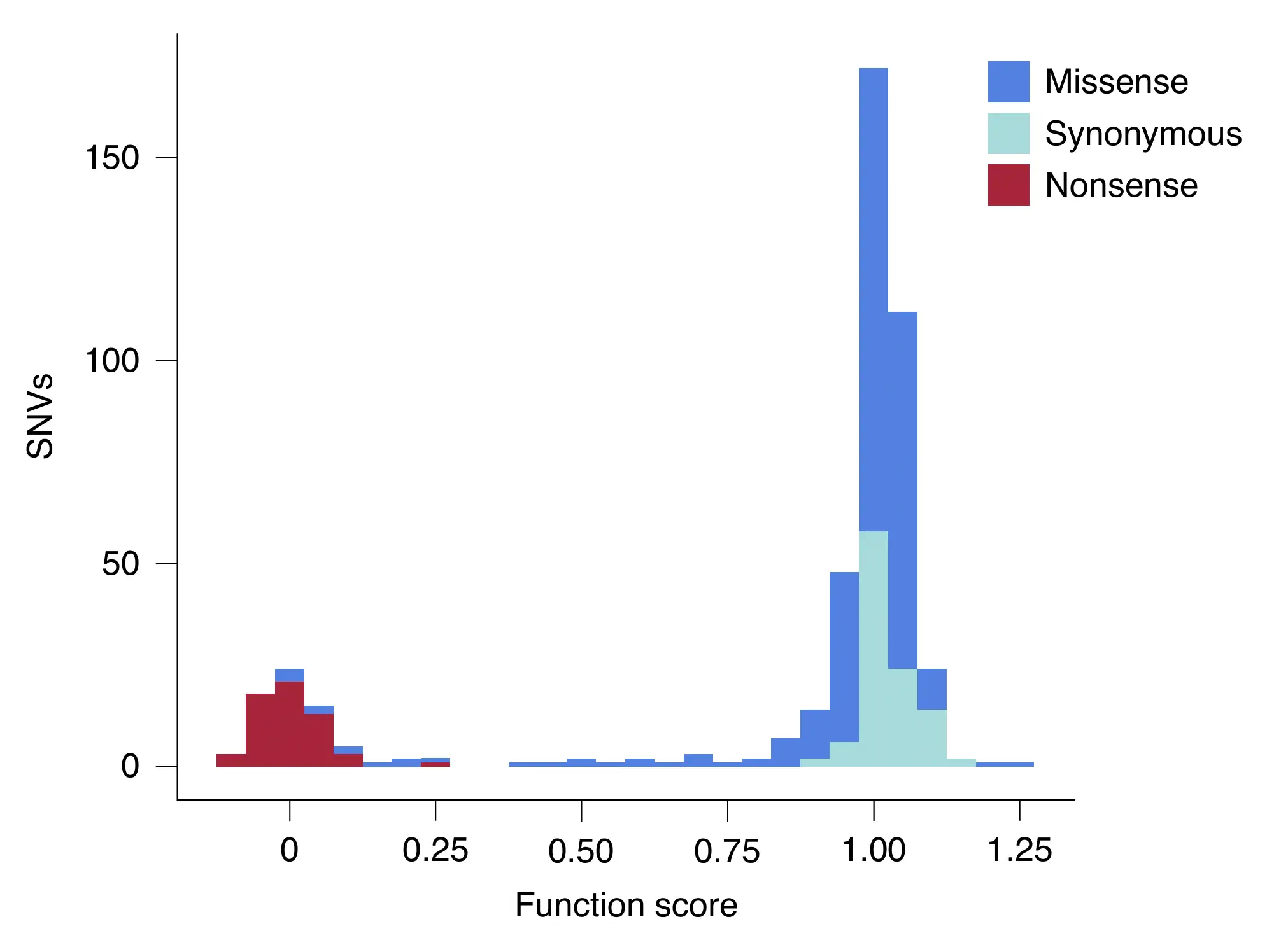
BRCA2 and PARP inhibitors
BRCA2 carries hundreds of variants of uncertain significance. PARP inhibitors are licensed for patients with clear loss-of-function variants, but the unclassified majority remain outside that label. Functional classification — scoring each variant for its effect on BRCA2 function and PARP-inhibitor sensitivity — converts that unclassified majority into actionable clinical data.
Standard geneSlice pipeline
Consultation → cell model development (~6 mo) → variant library and screening (~6 mo) → data delivery. Typically 6–12 months. See Technology.